Osseointegrated bone-anchors for securing a prosthesis in the hand
")
Our private Osseointegrated bone-anchors for securing a prosthesis in the hand services are provided at the Royal Free Hospital, Hampstead.
To find out more about our hospitals click here:
There are many patients who have lost a finger or thumb as a result of cancer or injury. In most cases, it is not necessary to replace the absent digit to improve function. However, the appearance of the hand is sometimes over-looked as an important part of hand function. In these cases, use of a silicone prosthetic replacement is sometimes a reasonable solution.
In order to secure a silicone prosthesis to the rest of the hand, it is necessary to have enough of a stump to allow this to be done securely – preferably without resorting to the use of straps or other encumbrances that would limit the cosmetic value of this solution. Typically, to secure a prosthetic digit to the hand, the residual stump has to be > 2.5 cm long. Any less than that, and the prosthetic digit will tend to fall off all the time. In such a situation, the prosthesis become more of an annoyance than a solution.
There are many ways to achieve a secure fixation between the prosthesis and the hand. However, one of the most elegant solutions is to use an osseointegrated bone-anchor. The Relimb service at the Royal Free have extensive experience with a variety of osseointegrated bone-anchors (made by different manufacturers) for use in the hand. However, our preferred implants are manufactured by Southern Implants (based in South Africa).
The bone-anchors are used to hold a silicone prosthesis onto the residual skeleton of the hand. Not only does this create a more secure point of fixation but it also creates the possibility that the silicone prosthesis will have some useful function since the patient can now apply more pressure to the end of the prosthesis. This makes it possible to carry out light duties such as typing or gripping small objects. However, it does not allow the user to carry out heavy duties such as mechanical engineering or building work.
Importantly, the surgery to place these bone-anchors is relatively simple (especially compared with the bone-anchors that are used for reconstruction after amputation of a limb). Moreover, the surgery can often be performed under local anaesthetic, although many patients prefer their surgery to be performed under a short general anaesthetic.
Planning:
Placement of the bone-anchors in the residual skeleton of the hand is critical. In theory, it should be possible to achieve sufficiently secure osseointegration to allow the bone-anchor to be used to fix a prosthetic digit in as little as 10 mm of bone. In practice, we would recommend at least 2.5 cm of fixation to avoid the unhappy situation of the bone-anchor pulling out. Importantly, unlike the craniofacial skeleton, it is usually necessary to place just one bone-anchor into the residual skeleton of the hand to secure a prosthesis.
Therefore, planning of a procedure and careful pre-operative assessment are a critical part of success. To plan the procedure, plain x-rays and (rarely) CT scans may also be needed. The surgeon will discuss your needs in clinic and a tentative plan will be made which may then need to be discussed with our prosthetic partners – before surgery is performed.
Procedure:
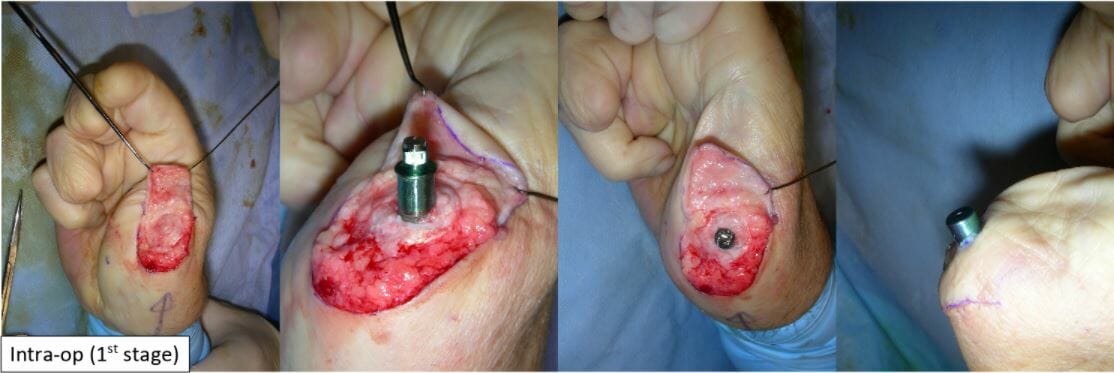
Surgery to place a bone-anchor in the hand is usually carried out in two stages. At the first stage, the end of your stump must be cleared off all soft-tissues. This can then be replaced with a thin split-thickness skin graft or skin flap which is applied to the adjacent periosteum. This ensures that the soft-tissues adjacent to the implant will become firmly adherent and will not (tend) to migrate over the transcutaneous parts of the bone-anchor – over the coming years.
Under image intensifier control, a bone-anchor is then placed inside the residual bone. The bone-anchors are then left in place to osseointegrate for a minimum of 6 weeks (3 months preferred).
After this, the second stage can be performed at which the transcutaneous abutments can be fitted. After another 6 weeks, the tissues will have settled, and you can be seen by our prosthetists for final fitting of your prosthesis.
Aftercare:
1st stage – At this stage, the bone-anchors are buried under a skin graft and there will not be much for you to see. Most of your aftercare is directed at looking after the skin graft. Fortunately, there is not much for you to do or see while the initial dressing is in place. Once this dressing is removed (typically at 1 – 2 weeks after surgery) you can start to shower your wound (but not soak in a bath). There are often many adherent crusts. These should not be picked-off. They should be allowed to fall off spontaneously. Eventually, after about 2 – 3 weeks, the skin graft will become stable enough to start moisturising it with simple Vaseline. Your skin graft donor site should have healed by this stage and can also be moisturised in the same way.
2nd stage – At this stage, you will see the transcutaneous abutments attached to the bone-anchor. The interface between the skin and the metal components is usually dressed with jelonet and gauze to absorb any exudate. After the first dressing change (at 7 to 10 days after surgery), you will not need to have another dressing applied. Instead, you should start to apply Savlon antiseptic ointment around the base of each abutment. You will need to continue using Savlon ointment in this way – for as long as the abutment remains in place. It will help to suppress any bacterial over-growth in the area and will keep things nice and clean.
Example